
More than 90,000 people in the United States are awaiting kidney transplants, with wait-times that can be five, seven, even 10 or more years, but new research from a team in the Perelman School of Medicine at the University of Pennsylvania, in partnership with Massachusetts General Hospital and other centers, show more options for cutting those wait times.
Transplanting kidneys from donors infected with hepatitis C virus (HCV)—organs often considered too risky to transplant—into patients without the virus, was shown to have promising outcomes in recent single-center studies. In 2016, a Penn Medicine team tested this approach and the use of an antiviral medication to eradicate HCV after transplant, which proved successful. Penn investigators have since applied the same approach to heart and lung transplantation. However, these results have never been replicated in multicenter trials.
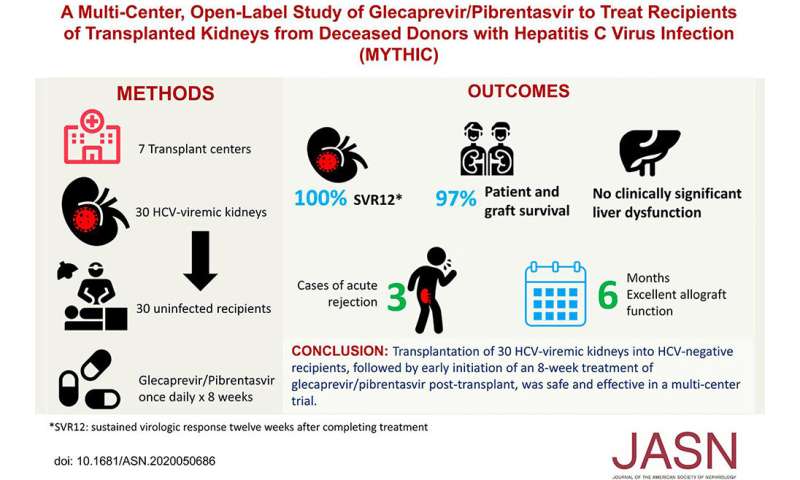
Now, results from the first multi-center trial of transplanting HCV-infected kidneys into uninfected recipients have been reported in the Journal of the American Society of Nephrology, showed the effectiveness of this approach in 30 HCV-positive kidney transplants.
“Transplant centers should take note of these results, which reveal an important opportunity for increasing access to kidney transplantation using kidneys that were often discarded in the past,” said senior author Peter Reese, MD, MSCE, an associate professor of Medicine and a nephrologist in the Penn Transplant Institute.
The collaborative team evaluated transplants in the trial conducted at seven medical centers from May to October 2019, and showed that all transplanted kidneys functioned well—and in every case HCV was undetectable in the kidney recipients after they completed a two-month course of the anti-HCV drugs—glecaprevir/pibrentasvir.
Reese, who led the transplant activities at Penn Medicine and coordinated data collection for the entire study team, worked with principle investigators at Massachusetts General Hospital Raymond Chung, MD and Meghan Sise, MD.
HCV, which is widespread across the world, can establish a chronic and largely silent infection, ultimately leading to liver failure or liver cancer. Needle sharing by users of heroin and other injectable drugs is a major route of HCV transmission, and so the opioid crisis in the U.S. is thought to have boosted the virus’s spread in recent years. The U.S. Centers for Disease Control and Prevention has estimated that in 2016 more than two million Americans were living with HCV infection.
The opioid crisis, with its rise in fatal overdoses, also has meant that many more Americans are dying with HCV infection. One recent study found that between 2010 and 2016 in the U.S., there was a nearly 300 percent increase in the number of organ donors who had died from drug overdose—and about one in every five of these donors had HCV infection. If it weren’t for the risk of HCV transmission, many of these donor kidneys would be considered very high quality, according to the researchers. The organs are generally younger, and therefore are less likely to have been damaged by age-related conditions such as diabetes and hypertension.
The development of antiviral drugs that can cure HCV infection in most patients over recent years has led transplant physicians to consider using these drugs to protect recipients of HCV-positive kidneys—thus effectively widening the pool of donor kidneys.
In this study, known as MYTHIC (Multicenter Study to Transplant Hepatitis C–Infected Kidneys), 30 HCV-uninfected patients who received kidneys from deceased, HCV-infected donors (median age 34) were evaluated. These patients were mostly on dialysis and otherwise would have faced, on average, multiple years of waiting for a “standard” HCV-negative kidney—but had a median wait-time of only about six weeks after they consented to receiving an HCV-positive kidney. The recipients were treated with a standard combination of anti-HCV drugs, glecaprevir/pibrentasvir, starting shortly after transplant.
The research team found that when tested, 12 weeks after finishing drug treatment, recipients had undetectable levels of HCV genetic material on sensitive blood tests, suggesting that the treatment had essentially cleared cured them of HCV and prevented a wider HCV infection from taking root.
Moreover, every one of the transplanted kidneys appeared to be functioning well, according to standard tests conducted six months after the transplants.
There were several serious adverse events among the 30 patients, including the death of one patient due to a bacterial infection nine months after transplant. But the researchers considered it unlikely that any of the adverse events was related to HCV infection or the anti-HCV treatment. Transplant recipients have a higher than normal risk of dangerous infections due to the immune-suppressing drugs they take to prevent transplant rejection.
The team concluded that transplanting HCV-positive kidneys while treating recipients with anti-HCV drugs is a safe and effective way to expand access to donor kidneys.
Source: Read Full Article