Obesity weakens heart muscle in patients with a common type of heart failure
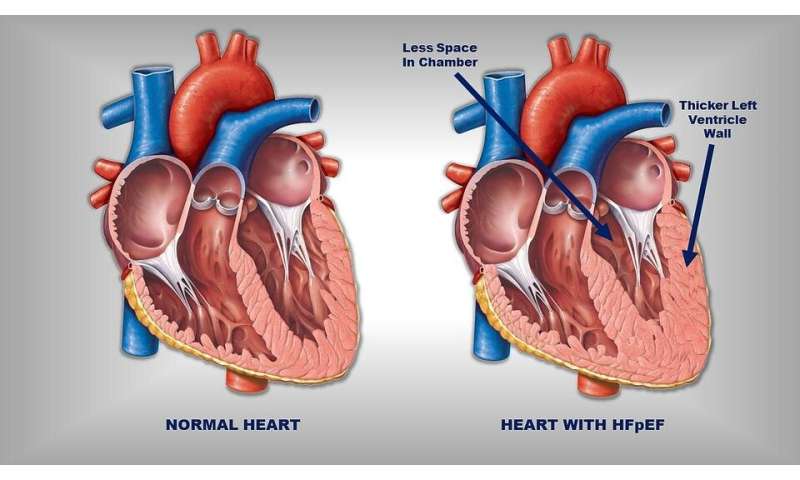
For decades, physicians have known that about half of all patients with heart failure appear to have hearts that contract normally—a syndrome now known as heart failure with a preserved ejection fraction (or HFpEF, pronounced hef-pef). This type of heart failure was first seen primarily in slim, elderly women with high blood pressures and thicker heart muscle. But as the incidence of obesity and diabetes has increased, many patients with HFpEF are now found to be severely obese with blood pressures not as high and heart muscle not as thick as seen in previous patients.
New research from Johns Hopkins Medicine has uncovered that greater obesity seems to make muscle contraction much weaker in this very common form of heart failure. In their study, published Dec. 2, 2020, in Circulation, the researchers say “the surprising findings upends the field,” as it challenges the view that the disease is all about having a stiff heart that cannot relax.
“Obesity would seem to have changed the heart muscle,” says senior study author David Kass, M.D., the Abraham and Virginia Weiss Professor of Cardiology at the Johns Hopkins University School of Medicine. “The “p” in HFpEF stands for preserved, and that’s what contraction was supposed to be, and what HFpEF used to be. But, as more patients are obese and our results show this reduces contraction strength, we will need to rethink our concepts and along with it, our treatments.”
Traditionally, this form of heart failure has been treated with medicines that often reduce contraction strength while improving the heart’s relaxation. Further research, Kass says, will need to determine if this approach needs to be modified.
Johns Hopkins Medicine has one of the few dedicated HFpEF clinics in the country, run by study co-author Kavita Sharma, M.D., associate professor of medicine and director of the heart failure transplant program at the Johns Hopkins University School of Medicine.
As part of the evaluation of patients with HFpEF, a tiny piece of heart muscle is collected using a standard heart biopsy procedure. The biopsy samples taken from patients who were less obese (a body mass index, or BMI, averaging 30) but had high blood pressure and thick heart muscle were compared with those with severe obesity (BMI averaging 40) but lower blood pressure and less thick heart muscle. The investigators teased out single muscle cells from these samples and studied their function. When the researchers added calcium to stimulate the cells to contract, those from the less-obese group responded normally.
However, the force response to high calcium was reduced by 40% in cells from patients with obesity. In a third group of patients who had both high blood pressure and thicker hearts, as well as severe obesity, the force response in the cells given calcium was similarly reduced as in the mostly obese group. Kass and his colleagues believe this points to obesity as the key factor.
HFpEF was previously called diastolic heart failure, emphasizing the idea that although the heart could contract normally, it didn’t properly fill with blood when the heart relaxed in preparation for the next beat (called diastole). While preserved contraction appears still true for less obese patients with high blood pressure and thick heart muscle, it doesn’t appear to hold true when they also have severe obesity.
Severe obesity alters underlying human biology—most recently brought in focus with the COVID-19 pandemic as obesity has been shown to be an independent risk factor for more severe disease and worse outcome. Many of COVID-19’s effects on artery function, the immune system and inflammation, and metabolism and heart stress may also be relevant to HFpEF, the researchers say.
Source: Read Full Article


